
PAMORA Treatment Suitability Guide
Analysis Results
Dealing with chronic pain often means trading one problem for another. You find relief from your discomfort, only to face stubborn constipation that refuses to respond to typical laxatives. This is the harsh reality for millions living with opioid-induced constipation (OIC). If you have tried stool softeners and bulk-forming fiber without success, there is a specialized class of medication designed specifically for your situation. These drugs, known as peripherally acting mu-opioid receptor antagonists, offer a targeted solution that stops the root cause rather than just treating symptoms.
In 2026, managing this side effect is more nuanced than it was five years ago. We have better options, clearer guidelines on safety, and access to newer formulations that might fit your lifestyle. However, knowing which agent to choose requires understanding how they differ, not just their names. Let's break down exactly what these medications are, who they help, and what to expect when you start using them.
Opioid-Induced Constipation Defined
Opioid-induced constipation (OIC) is a distinct type of bowel dysfunction caused by opioids binding to receptors in the gut wall. Unlike common constipation, which might happen due to low fiber intake, OIC occurs because opioids slow down the entire gastrointestinal system. About 40 to 80 percent of patients taking long-term opioids develop this issue. It doesn't just mean infrequent bowel movements; it often involves hard stools, straining, abdominal bloating, and even nausea.
The mechanism is straightforward but frustrating. When you take an opioid for pain, the medication travels through your body. While it binds to receptors in your brain to dull pain signals, it also binds to receptors in your intestines. These intestinal receptors tell the gut to stop moving. Regular laxatives often struggle here because they don't reverse the opioid's chemical hold on the gut muscles. Studies show that traditional stool softeners maintain regular bowel function in fewer than 30 percent of chronic users.
How PAMORAs Break Through the Blockade
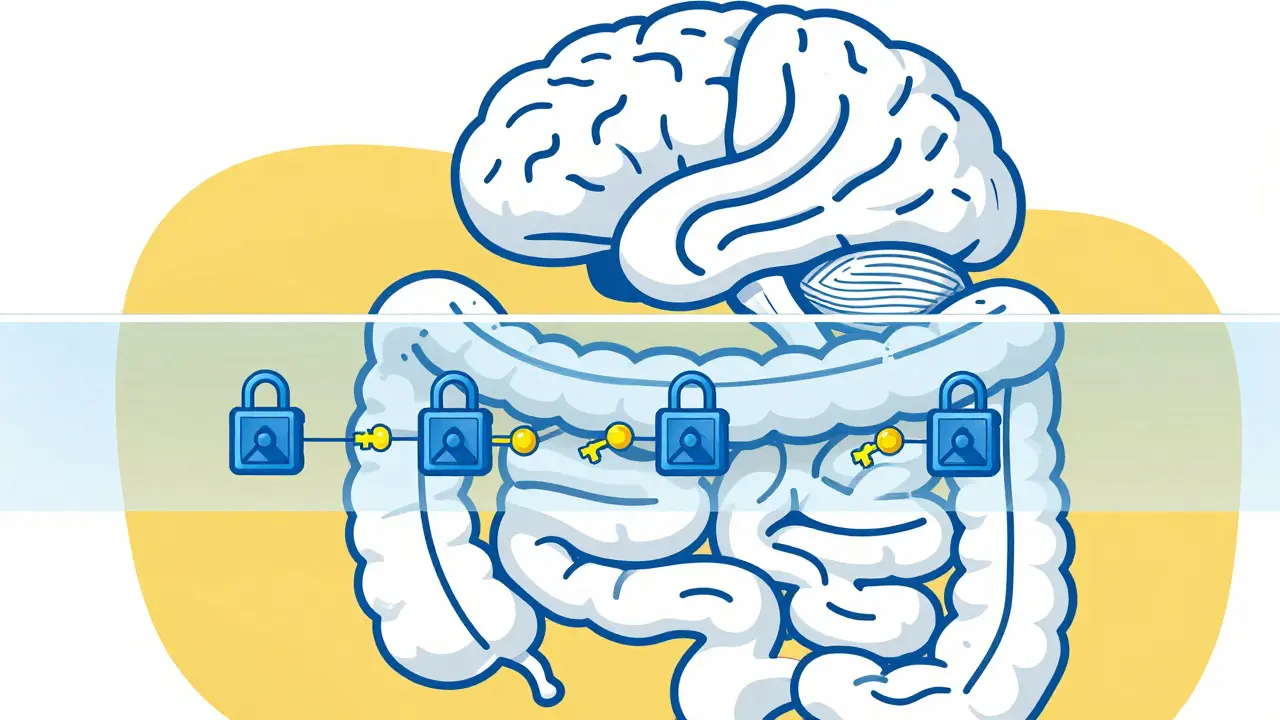
PAMORAs is short for Peripherally Acting Mu-Opioid Receptor Antagonists, a drug class that selectively blocks opioid effects outside the brain. Think of it like having two keys for one lock. Your pain medication uses the key to turn off the pain signal. PAMORAs act as a blocker that fits the same lock in your gut but won't fit the locks in your brain.
This selectivity relies on a biological feature called the blood-brain barrier. Most PAMORAs are engineered to be too heavy or charged to pass through this protective shield. They remain in the bloodstream and tissues of the abdomen, reversing the slowdown in motility while keeping your analgesia intact. This is crucial because stopping pain medication just to fix bowel issues usually isn't an option for patients.
Mechanically speaking, these drugs bind to the mu-opioid receptors in the enteric nervous system. By occupying these spots, they prevent the opioids you are taking for pain from activating them. Once blocked, the gut resumes normal movement. Clinical trials indicate that roughly 52 percent of patients achieve a bowel movement within four hours of taking certain agents, compared to just 30 percent on placebo.
Available Medications: Comparisons
You will likely encounter three main brand names when discussing treatment plans with your doctor. Each has slightly different properties regarding how it is taken and absorbed. Understanding these differences helps you pick the right partner for your daily routine.
| Drug Name | Common Brand | Administration Route | Dosing Frequency | Key Distinction |
|---|---|---|---|---|
| Methylnaltrexone | Relistor | Subcutaneous Injection / Oral Tablet | As needed or Twice weekly | Fastest onset (under 4 hours); Available in both forms |
| Naloxegol | Movantik | Oral Tablet | Once Daily | Long half-life (8-13 hours); Good for scheduled relief |
| Naldemedine | Symproic | Oral Capsule | Twice Daily | Takes 2-3 days to reach full effect; Requires food |
| Alvimopan | Entereg | Oral Capsule | Post-operative only | Hospital use only; Restricted distribution program |
Methylnaltrexone remains the most versatile option. Originally approved in 2008, it works rapidly. If you feel blocked up suddenly, a subcutaneous injection can clear things out much faster than a pill. Recent approvals in early 2023 added a higher strength oral tablet (300 mg) for severe cases that didn't respond to standard doses. However, it requires monitoring for kidney function, especially if you have renal impairment.
Naloxegol functions similarly but comes only as a once-daily pill. It is pegylated, meaning it has a polymer chain attached to restrict it further to peripheral tissues. It is metabolized by a specific liver enzyme called CYP3A4, so interactions are possible with other strong meds. Response rates were around 44 percent in phase 3 trials over 12 weeks. It is generally preferred for patients who want a set-and-forget daily schedule rather than injections.
Naldemedine takes a slightly longer approach. Because it reaches peak plasma levels later, it might take a few days of consistent use before you see the full benefit. It is useful for those who prefer avoiding needles and don't mind a loading period. Clinical data shows a response rate of nearly 48 percent against placebo.
A fourth option, Alvimopan, exists primarily for hospital settings. It helps accelerate recovery after bowel resection surgery. Due to potential cardiovascular risks seen in long-term use during early trials, the FDA placed strict limits on its distribution. You typically won't prescribe this for home maintenance care.
Real-World Usage and Challenges
Knowing the science is one thing; living with the treatment is another. When looking at patient feedback forums, effectiveness varies by individual biology. For instance, some cancer patients report that methylnaltrexone significantly improved quality of life without interfering with pain control. Others mention severe abdominal cramping shortly after taking the medication. Roughly 32 percent of negative reviews cite cramping as the primary reason for stopping therapy.
Cost is a major hurdle in 2026. Without insurance support, annual costs can exceed $6,000. Manufacturer coupons exist, but navigating prior authorizations with payers takes time. You should prepare your prescriber to handle these administrative tasks upfront. Insurance companies often require a documented trial of traditional laxatives first before approving PAMORAs. Keep a log of your bowel movements and laxative usage for at least a month before requesting approval.
Timing matters immensely. The optimal window appears to be dosing about one hour before your pain medication peaks. This preemptive strike ensures the antagonist is ready to block the receptor before the opioid does. Missing this window or taking doses inconsistently reduces efficacy. Renal adjustments are also critical; if your creatinine clearance drops below 30 mL/min, dose reductions are mandatory to avoid toxicity.
Who Should Not Take These Medications
Safety dictates strict contraindications for this class. You cannot take PAMORAs if you have a suspected mechanical obstruction in your gut. Since the drug forces the gut to move, doing so when a blockage exists could rupture the intestine, leading to a surgical emergency. Signs of obstruction include sudden vomiting, inability to pass gas, and severe distension. Your doctor must screen for this history before starting therapy.
Pregnant individuals should also avoid these drugs unless absolutely necessary, as placental transfer could trigger withdrawal symptoms in a fetus. Additionally, severe hepatic impairment poses risks with agents like naloxegol, where dose reduction or contraindication depends on severity grading.
Monitoring Success and Adjusting Care
You need to define what "success" looks like for you. Usually, this means achieving two or more spontaneous bowel movements per week without straining. Track your progress for the first three months. If the medication stops working after an initial response-something reported in forums like Healthgrades-it might be time to rotate agents. Some patients find switching from naloxegol to methylnaltrexone restores responsiveness.
If side effects persist despite good tolerance of the drug, talk to your specialist about combining strategies. Sometimes, adding a lower-cost adjunct like lubiprostone alongside the PAMORA improves results. As we look toward the future, researchers are testing combination therapies, including dual-action molecules that target serotonin pathways simultaneously, showing promising response rates in recent Phase 2 trials funded by the NIH.
Will PAMORAs reduce my pain relief?
Because these drugs cannot cross the blood-brain barrier effectively, they should not interfere with your pain control. However, small studies suggest up to 60 percent of analgesia has a peripheral component, so monitor your pain levels closely if you notice changes.
How quickly do these medications work?
Injectable methylnaltrexone works fastest, often inducing bowel movement within 4 hours. Oral options like naloxegol or naldemedine may take days of consistent dosing to reach full therapeutic effect.
What should I do if I experience abdominal cramping?
Cramping is a common side effect. If it becomes severe, discontinue use and contact your provider immediately, as it could signal an obstruction. Mild cramps often resolve as your body adjusts over the first few doses.
Can I use these drugs long-term?
Yes, they are indicated for chronic use. Long-term safety data supports continued administration in palliative care and non-cancer pain scenarios, provided renal and hepatic functions are monitored regularly.
Are there generic versions available yet?
Biosimilar versions are currently entering late-stage trials globally. While patents still cover many original brands, expect more competition and price shifts to emerge by 2028.
Comments
Tony Yorke March 28, 2026 at 05:57
Mechanism explains why standard stool softeners frequently fall short
Jeannette Kwiatkowski Kwiatkowski March 28, 2026 at 23:30
Most people just take senna and complain when it does not work instead of reading the pharmacology involved
Aaron Olney March 29, 2026 at 12:28
Peepz dont get it they r stuck in pain and need help right now not lecture on mehds lol
Sabrina Herciu March 31, 2026 at 06:45
It is vital to note that renal function dictates dosing! You cannot ignore creatinine clearance levels!! Safety first always!!!
Rachael Hammond March 31, 2026 at 23:57
yeah shees true i always forget the kidney part until my doctor brings it up thanks for reminding peepz
tyler lamarre April 1, 2026 at 15:41
another drug class for people too lazy to drink water and eat fiber naturally just pay me back later
Sarah Klingenberg April 2, 2026 at 03:31
chronic pain isnt always about being lazy tyler some meds do this regardless of diet try to be kind 🙂
Richard Kubíček April 3, 2026 at 07:09
Selective antagonism allows pain relief to persist while bowel movement returns to normal rates. Many patients assume blockers reduce analgesia but that is not typically observed clinically. Modern pharmacology distinguishes between central and peripheral receptor blocking effectively. We need more education like this to stop stigma around managing side effects. My uncle struggled with constipation for years before finding these options. He was afraid to talk about bowel issues with his oncologist. Fear often stops us from seeking the help we deserve during treatment. Cost remains a huge barrier unfortunately for those without insurance support. Manufacturers need to step up their assistance programs for sure. Waiting months for approval is painful enough without adding financial stress. The timing advice about taking meds before opioid peaks is something many miss. Consistency seems to be the real key here alongside the actual medication choice. Side effects like cramping do taper off over time usually after the first week. Patience is definitely required when starting something new like methylnaltrexone. Switching agents is totally viable if one just stops responding eventually. Life quality matters far more than stubbornly sticking to a failing regimen forever. Hope everyone finds relief soon through proper guidance.
Philip Wynkoop April 4, 2026 at 13:07
great point about consistency 😊 costs are rough though
Shawn Sauve April 5, 2026 at 02:39
Really useful guide on the different options out there 🙌
Debra Brigman April 6, 2026 at 04:06
The symphony of gut motility requires such delicate tuning indeed our internal rhythms dance to chemical cues