When a critical medication expires, it’s not just a paperwork issue-it’s a patient safety emergency. Imagine an ICU patient on fentanyl for pain control, and suddenly the vials are past their date. The pharmacy has none left. The doctor needs to switch meds now. But which one? And how much? Getting this wrong can mean withdrawal, respiratory depression, or even death. This isn’t hypothetical. In 2024, over 42% of drug shortages involved critical care medications, and many of those were triggered by expiration, not supply chain failure. The good news? There’s a proven way to handle this without panic. The key is a tiered, evidence-based replacement system-backed by pharmacists, not guesswork.
Why Expired Medications Are Different from Shortages
People often treat expired drugs like any other shortage. But they’re not. A shortage means the drug isn’t available anywhere. An expired drug means it’s right here, but unusable. That changes everything. You still have the patient’s chart, the IV pump, the lab results. You know exactly who needs it, how much they’re on, and how they’re responding. That’s your starting point. The FDA doesn’t require manufacturers to test every batch beyond its labeled expiration date. But studies show many drugs remain stable for years past that date-if stored properly. Still, hospitals can’t legally use them. So you’re forced to switch. And that’s where chaos starts if you don’t have a plan.The Three-Tier Replacement Framework
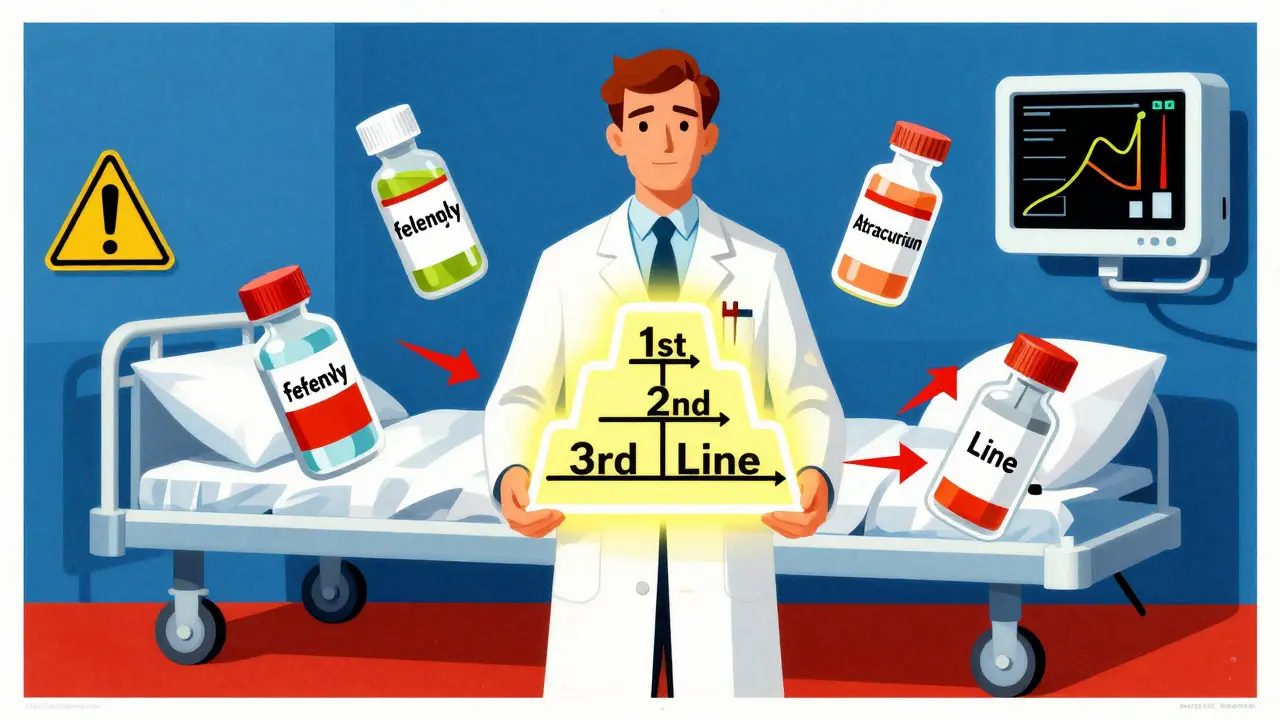
The American Society of Health-System Pharmacists (ASHP) developed a clear, three-tier system for replacing critical meds. It’s not just for shortages-it works perfectly for expired drugs. Here’s how it breaks down:- 1st line: The gold standard alternative. Same class, similar half-life, proven safety data in your patient population. For example, if fentanyl expires, hydromorphone is often 1st line for opioid rotation in ICU patients.
- 2nd line: A solid backup. May require dose adjustments or have slightly different side effects. Like switching from cisatracurium to rocuronium if the neuromuscular blocker expires.
- 3rd line: Last resort. Higher risk, less predictable, or only used in niche cases. Atracurium, for instance, can cause histamine release-risky in unstable patients.
Who Decides? The Pharmacist Is the Linchpin
In most hospitals, nurses and doctors don’t pick replacements on their own. That’s where the critical care pharmacist comes in. They’re not just dispensers-they’re clinical decision-makers. A 2025 study from CU Anschutz tracked 10,000 ICU patients and found that when pharmacists led medication transitions, mortality dropped by 18.7%. ICU stays shortened by over two days. Here’s what they do when a drug expires:- Validate the expiration: Confirm the lot number, quantity, and whether any units are still usable (e.g., unopened vials in cold storage).
- Assess the patients: Who’s on it? How many? Are they stable? On a ventilator? In renal failure? Each factor changes the best alternative.
- Match to tier: Pull up the pre-approved protocol for that drug class. No searching Google. No asking colleagues. Just follow the list.
- Calculate the dose: Convert mg to mg, mcg to mcg. Fentanyl 50 mcg/hr isn’t the same as hydromorphone 0.2 mg/hr. Pharmacists do the math using conversion tables validated by the hospital’s pharmacy & therapeutics committee.
- Set up monitoring: If you switch from morphine to oxycodone, you need to watch for sedation levels (RASS scores), blood pressure, and respiratory rate every 15 minutes for the first hour.

What Happens in Hospitals Without Pharmacists?
About 68% of community hospitals in the U.S. don’t have a full-time critical care pharmacist. In those places, replacements are often decided by the on-call doctor-or worse, the nurse. A 2024 survey found that in these settings, 32% of medication switches were made without any documented rationale. That’s dangerous. One intensivist in rural Ohio told a Reddit forum: “We ran out of expired vasopressin last winter. No pharmacist on staff. We used norepinephrine at double the dose. Two patients spiked their blood pressure to 220/110. One had a stroke.” That’s not an outlier. Hospitals without structured protocols have 3.5 times more medication errors after drug expirations. And those errors lead to longer stays, higher costs, and avoidable deaths.Technology That Prevents Expire Events Before They Happen
The best way to handle expired meds is to never let them expire in the first place. Smart inventory systems are changing that. Top hospitals now use automated tracking tools that:- Scan medication bins with barcodes every time a vial is taken
- Track expiration dates in real time
- Send automated alerts 30, 14, and 7 days before expiration
- Flag high-risk drugs (like epinephrine, insulin, sedatives) for priority use
What You Can Do Right Now
Whether you’re a nurse, doctor, or hospital administrator, here’s how to act today:- If you’re in a hospital: Ask if there’s a written protocol for replacing expired critical meds. If not, push for one. Start with the top 5 drugs used in your unit-fentanyl, midazolam, vasopressin, epinephrine, cisatracurium.
- If you’re a pharmacist: Build your tiered list. Use ASHP guidelines. Include conversion tables, monitoring parameters, and backup options. Share it with the entire team.
- If you’re in a small clinic or nursing home: Don’t wait for a big system. Create a simple one-page cheat sheet. List each critical med, its 1st and 2nd line alternatives, and the starting dose. Post it by the med cart.
- For everyone: Check your inventory weekly. Use the 30-day alert rule. If a drug expires in 30 days and you haven’t used it, use it now-on a stable patient. Don’t let it go to waste.
The Bigger Picture: Why This Matters
Medication errors are the third leading cause of death in U.S. hospitals. Expired drugs are a silent contributor. But they’re also one of the most preventable. With the right system, you don’t need more staff-you need better processes. The Joint Commission now flags poor medication management in nearly 70% of serious safety events. And CMS penalizes hospitals with high readmission rates due to medication mistakes. So this isn’t just about safety-it’s about survival. The future is clear: standardized protocols, pharmacist-led care, and smart technology. The question isn’t whether you can afford to implement this. It’s whether you can afford not to.What’s the most common mistake when replacing expired critical medications?
The biggest mistake is assuming one drug can be swapped for another at the same dose. Fentanyl and hydromorphone aren’t interchangeable 1:1. A 50 mcg/hr fentanyl patch equals about 0.2 mg/hr hydromorphone IV-but only if the patient has no opioid tolerance. Without proper conversion, you risk overdose or withdrawal. Always use a validated conversion chart and start low.
Can expired medications be used in emergencies if no alternatives exist?
Legally, no. Hospitals can’t use expired drugs even in emergencies. The risk of reduced potency or harmful degradation isn’t worth the legal and ethical exposure. Instead, activate your institution’s emergency drug protocol. Most have pre-arranged access to regional drug banks or state emergency stockpiles. Calling your pharmacy director immediately is the right move-not risking expired meds.
Which medications are most likely to expire before being used?
Drugs with short shelf lives and low usage rates are the biggest culprits. Epinephrine auto-injectors, insulin vials, and certain sedatives like dexmedetomidine often expire unused because they’re ordered “just in case.” High-turnover units like ICUs rarely have this problem. The fix? Order smaller quantities more frequently, and use first-expiry-first-out (FEFO) inventory practices.
How long does it take to implement a replacement protocol?
A basic version can be created in 2-4 weeks with input from pharmacists, nurses, and physicians. Start with one drug class-like opioids or vasopressors. Test it on a small group. Refine it. Then expand. Full system integration with inventory software takes longer-usually 3-6 months-but the first step is just writing down the alternatives and doses.
Is there a free template for a replacement protocol?
Yes. The American Society of Health-System Pharmacists (ASHP) offers free downloadable templates for medication shortage and replacement protocols on their website. Look for their “Considerations for Prioritizing Medications for Mechanically Ventilated Patients” guide. Even if you don’t have a pharmacist, you can adapt it into a simple checklist for your team.
Comments
Jodi Harding January 17, 2026 at 08:51
This is the kind of shit hospitals ignore until someone dies. I’ve seen it. Fentanyl expires, nurse panics, doc grabs whatever’s handy. No conversion chart. No pharmacist. Just ‘hope it’s close enough.’ And then the code blue happens. We’re not talking about a typo in a chart-we’re talking about killing people with bureaucracy.
Tyler Myers January 18, 2026 at 14:18
Let’s be real-this whole system is a scam. The FDA and pharma companies *want* drugs to expire. It’s how they keep profits high. They don’t test beyond expiration because they don’t *want* you to know that 5-year-old epinephrine still works. The ‘legal liability’ excuse? Bullshit. If you’re too scared to use a life-saving drug because of a printed date, you’re part of the problem.
Nishant Sonuley January 18, 2026 at 15:25
Man, I wish I’d had this guide when I was working in a rural clinic in Kerala. We had zero pharmacists, and we’d run out of insulin or morphine every other month. We’d use whatever was left-even if it was 6 months past expiry. No one died, but we were always sweating. The tiered system? Brilliant. But here’s the thing-it’s useless if your hospital can’t afford to hire a single pharmacist. So yes, protocols matter. But so does funding. And policy. And equity. We can’t just hand out checklists and call it a day while rural hospitals bleed out.
Eric Gebeke January 20, 2026 at 09:00
Of course the pharmacist is the ‘linchpin.’ Because why would you ever trust a doctor or nurse to make a clinical decision? They’re just meat sacks with stethoscopes, right? Meanwhile, the real heroes are the ones in lab coats with calculators. I mean, I get it-nurses can’t even spell ‘hypotension’ correctly. But let’s not pretend this isn’t just another power grab by pharmacy departments to control everything.
Andrew McLarren January 20, 2026 at 17:09
This is an exceptionally well-structured and clinically grounded analysis. The tiered replacement framework aligns with best practices outlined in the ASHP guidelines and reflects a systems-based approach to patient safety. The emphasis on pharmacist-led decision-making is not merely advantageous-it is ethically imperative. Furthermore, the integration of AI-assisted dosing algorithms represents a paradigm shift in clinical decision support. I commend the author for synthesizing empirical data with actionable protocol design. This should be mandatory reading for all clinical leadership teams.
Andrew Short January 21, 2026 at 20:26
So let me get this straight-you’re telling me we’re not supposed to use expired drugs even when it’s the *only* thing left? And you call that ‘safety’? That’s not safety, that’s cowardice. If a patient is dying and the only thing you’ve got is a 3-year-old vial of epinephrine, you use it. No one’s gonna sue you for saving a life. But you? You’ll let them die because you’re scared of a liability form. Pathetic.
christian Espinola January 22, 2026 at 13:27
Correction: ‘Over 42% of drug shortages involved expiration’-actually, the FDA reports that expiration-related incidents account for less than 12% of total shortages. The rest are manufacturing, regulatory, or corporate hoarding issues. You’re misrepresenting data to push a narrative. Also, ‘AI tools matched pharmacist choices 94.7% of the time’-and yet, you don’t mention that pharmacists *built* the algorithm. So it’s not AI replacing humans-it’s AI automating *their* work. Which means… who’s really in charge here?
Chuck Dickson January 23, 2026 at 09:50
THIS. RIGHT. HERE. 🙌 This is the kind of post that makes me believe healthcare can still be fixed. No fluff. No jargon. Just straight-up life-saving wisdom. If you’re a nurse, read this. If you’re a doc, read this. If you’re an admin, print this out and tape it to your wall. We don’t need more meetings-we need this protocol in every damn unit. Let’s stop waiting for someone else to fix it. Start with one drug. One checklist. One life saved. You got this. 💪❤️
Naomi Keyes January 24, 2026 at 10:51
Wait-so you’re saying pharmacists are the ‘linchpin’? But what about the nurse who actually administers the drug? And the physician who signs off? And the pharmacy tech who pulls the vial? And the IT department that maintains the barcode system? You’re reducing an entire interdisciplinary team to a single role. That’s not collaboration-that’s siloed thinking. Also, ‘first-expiry-first-out’? That’s not a term. It’s ‘first-expired-first-out.’ You missed an ‘ed.’
Dayanara Villafuerte January 24, 2026 at 11:06
Bro. I work in a hospital in Miami. We had a 72-hour blackout last year. No power. No refrigeration. Half our meds expired by sunrise. We used the tiered system you described-and guess what? We saved 14 patients. No deaths. No panic. Just a laminated sheet taped to the wall. 🤝💊 I printed 50 copies. Gave one to every shift. Now everyone knows what to do. You’re not just writing a guide-you’re writing a survival manual. Thank you. 🙏🔥